
Exfoliating Cream vs. Professional Peel: Understanding the Clinical Difference
Many cosmeticians ask during trainings: what is the difference between a cream containing hydroxy acids and an in-clinic peel with the same acid concentration? And do we really need both? After all, there are products on the market with 16% alpha hydroxy acids for home use, and professional peels at the same concentration used in the clinic. The same percentage and let us assume even the same pH. In reality, that is often not the case, but for the sake of discussion, let us assume it is. Theoretically, we might expect a similar effect. In practice, the skin response is completely different.
In a cream, the acids function within a full emulsion system that contains lipids, humectants, and sometimes barrier-supporting or reparative ingredients. From the skin’s perspective, this means a slower release of the acids into the stratum corneum, a more gradual and cumulative action, and at the same time preservation of the epidermal barrier. The cream provides a certain degree of occlusion, softens the stratum corneum, reduces transepidermal water loss, and allows progressive penetration while maintaining the integrity of the intercellular lipid structure. There is no sharp barrier disruption and no significant biological stress, which is why professional active creams can be prescribed for home use, of course only after proper skin assessment and with personalized instructions. It is an excellent tool for safe renewal, daily maintenance, regulation of cell turnover, and gradual improvement of texture and tone. Can a cream produce visible results in a relatively short time? Yes, especially if it is highly active. But it does not create the same level of exfoliative impact as a professional in-clinic peel. It builds a process.
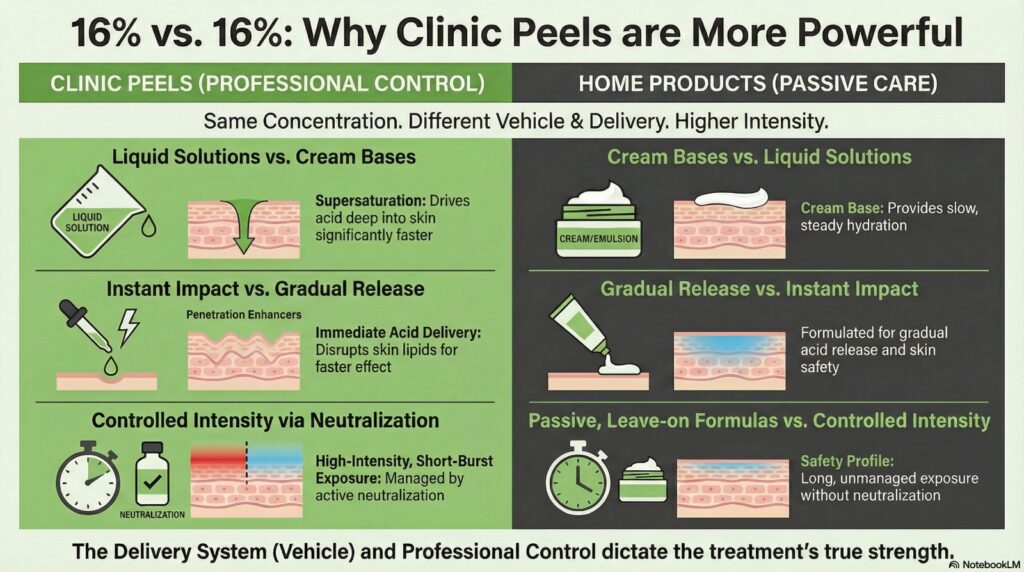
In an in-clinic peel, particularly a liquid formula and especially one that contains alcohol, the conditions are different. There is no protective lipid system and no occlusion. The stratum corneum is directly exposed to the acid. A temporary alteration of the lipid structure occurs, along with a sharp increase in permeability. This rapid penetration generates controlled stress that activates repair mechanisms, accelerates cell turnover, and produces more significant renewal within a short time frame. We are essentially creating a controlled, short-term chemical injury. This is precisely why full professional supervision is required. We control exposure time, we respond in real time to the skin’s reaction, and we can work selectively on specific areas, for example using an applicator to target pigmentation or other aesthetic concerns. It is a sharp intervention, performed occasionally rather than daily or even weekly, capable of producing a clear therapeutic leap after a single session.
So is it enough to use only one of them? For example, to rely solely on a good professional cream, or only on in-clinic peels? The short answer is no. If we rely only on a cream, we achieve a safe, gradual, ongoing process, but without the accelerated biological stimulus that significantly boosts renewal and allows precise work on localized concerns such as pigmentation. Everything progresses more slowly and with less depth of impact. The clinical peel acts as a true engine of change. On the other hand, if we perform clinical peels without structured home care, we create periodic stress but lose the ability to consolidate and maintain the results. The skin is a dynamic system that constantly strives for equilibrium. It responds to stimulation, but it also returns to its baseline patterns. Clinical thinking is therefore not about choosing between a cream and a peel. It is about understanding at which stage in our therapeutic protocol a sharp, controlled renewal is required, and at which stage a quiet, daily process is needed to stabilize and preserve the improvement. This is where our professional judgment becomes essential.